5 Facts About Understanding Pain
The Following Extract was Written for the Australian Physiotherapy Association by Dr Tania Gardner. Dr Gardiner is an APA Pain Physiotherapist and senior physiotherapist in the Department of Pain Medicine, St Vincent’s Hospital Sydney.
1. Understand pain
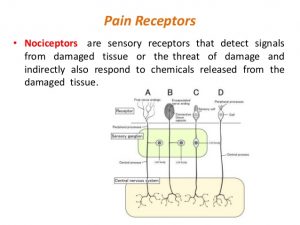
 Pain is a normal human experience. Its purpose is one of protection—to alert us of potential harm so that we can respond to minimise damage and facilitate healing.
Pain is a normal human experience. Its purpose is one of protection—to alert us of potential harm so that we can respond to minimise damage and facilitate healing.
In the acute situation, responses such as limiting movement, increasing muscle activity to protect an injured area and increasing awareness of nociception (pain perception) through adaptive central (brain) sensitisation, may initially be useful protective behaviours.
However, often when pain becomes chronic, it is not a signal of ongoing tissue damage requiring protection. Cognitive and contextual factors may play an increased role in the pain experience, contributing to prolonged sensitivity. The reason why the system remains sensitised is multifactorial, and science is still investigating those factors. Chronic pain is complex with many interrelated components, and so prevention of it requires a multimodal approach.
In an acute pain situation, physiotherapists can steer patients towards a successful outcome by performing a thorough examination using language that does not increase catastrophising or fear of movement (ie, these are risk factors for the development of chronic pain).
Helpful interpretation of radiological findings, encouragement to stay active, targeted reassurance and pain education can be integrated into all person-centred management approaches of acute pain that a Physio will help patients with.
2. Early screening for risk factors
 There are numerous factors that are now known to increase the likelihood of transitioning to chronic pain. These include cognitive factors (eg, catastrophising and pain beliefs), mood (eg, depression and anxiety) and approaches to coping (eg, utilisation of more passive strategies, ie “someone or something will fix me” thoughts and actions).
There are numerous factors that are now known to increase the likelihood of transitioning to chronic pain. These include cognitive factors (eg, catastrophising and pain beliefs), mood (eg, depression and anxiety) and approaches to coping (eg, utilisation of more passive strategies, ie “someone or something will fix me” thoughts and actions).
Screening by a Physio for these factors can commence with careful attention to the patient’s story during the initial assessment and with appropriate pain questionnaires.
Screening tools such as the Orebro Musculoskeletal Pain Questionnaire can assist with the early identification of risk factors and guide appropriate treatment. Other measures such as the Pain Catastrophising Scale; Tampa Scale of Kinesiophobia; the Depression, Anxiety and Stress Scale; and the Pain Self Efficacy Questionnaire are all freely available to download and are useful as both screening tools and outcome measures.
When risk factors are identified, individualised early management including education, graded activity and other psychological interventions (as required) may facilitate a shift in patients’ beliefs and attitudes, and reduce fear and anxiety. Education about pain should encourage a reconceptualisation of pain—that it is not necessarily a marker of tissue damage, but that it is a protective response influenced by multiple factors, so affording us some control over this output.
3. Exercise regularly
 Physiotherapists are ideally placed to provide education & direction regarding the benefits of exercise and how this relates to chronic pain. Physical activity and exercise have broad positive health benefits due to their impact on the musculoskeletal, cardiovascular, immune and central nervous systems.
Physiotherapists are ideally placed to provide education & direction regarding the benefits of exercise and how this relates to chronic pain. Physical activity and exercise have broad positive health benefits due to their impact on the musculoskeletal, cardiovascular, immune and central nervous systems.

Physical activity is known to reduce pain intensity, fatigue, functional disability as well as provide a range of other benefits including improvements in strength, flexibility and endurance, a decrease in cardiovascular and metabolic syndrome risk, improved bone health and improved cognition and mood.
Physical activity can help to improve the level of function in daily and work-related activities, mental health and quality of life.
Physical activities and exercises may also be considered a valuable mental health promotion strategy in reducing the risk of developing mental health disorders, which are frequently associated with chronic pain.
Evidence suggests that exercise helps to prevent chronic neck and low back pain. The type of exercise does not seem to matter, with no exercise mode superior to another, meaning any movement or activity will be helpful. With that in mind the exercise that is chosen should be something that an individual is interested in and enjoys.
Outcomes will be best when the activity is something that is related to the patient-led goals.
4. Adopt Immune-boosting strategies
 The role of the immune system in the development and maintenance of chronic pain has gained attention with low-grade inflammatory biomarkers supporting an underlying inflammatory process in conditions such as osteoarthritis, low back pain, neck pain and radicular (leg/arm pain originating from the spine).
The role of the immune system in the development and maintenance of chronic pain has gained attention with low-grade inflammatory biomarkers supporting an underlying inflammatory process in conditions such as osteoarthritis, low back pain, neck pain and radicular (leg/arm pain originating from the spine).
Inflammatory biomarkers have also been observed to be associated with psychological and social factors. Therefore, immune-boosting strategies through attention to diet, sleep and stress are appropriate.
Certain foods seem to help reduce inflammation and protect the body from oxidant damage; polyphenols (compounds found in fruit and vegetables) have anti-oxidant and anti-inflammatory properties, while good-quality fats (such as Omega-3 fats and olive oil) reduce inflammation and enhance the immune system. A Consult with an Accredited Sports Dietitian can help patients with this pathway.
Sleep is a risk factor for chronic pain, and studies have suggested that addressing sleep problems may lessen the risk of developing depressive illness that is associated with a poor pain prognosis.
Emotional factors can contribute to the development or maintenance of prolonged sensitisation in chronic pain. Managing stress can help to reduce pain through multiple mechanisms (eg, reduced muscle activation, enhanced descending inhibition and reduced fear). Mindfulness, meditation, deep breathing and exercise are all ways to reduce the influence of stress.
5. Seek counsel or psychological/ behavioural therapy when needed
All physiotherapists use some form of psychological strategies in their treatment approaches. However, they do have a scope of practice & Referral to a psychologist working in chronic pain is recommended either when stress and mood disorders interfere with regaining everyday function or when more serious psychological disorders are suspected.
Anxiety, depression, anger, irritability and stress can all affect how the nervous system works. If these emotions are not well managed, the chances of developing chronic pain are increased.
Effective management and prevention of pain often requires patients to gain greater awareness and new skills to engage with a meaningful life more successfully. Clinical psychologists can help work through this process. Behavioural and cognitive interventions have been found to be effective in reducing pain and disability in many pain conditions, often with physiotherapists and clinical psychologists working collaboratively.
Treating the whole person in a biopsychosocial framework is crucial when treating pain.
If you need help managing YOUR PAIN, Consult with One of our Team of experienced Physiotherapists, Dietitian or Psychologist. Ph 07 55006470 for an appointment or Book Online.
Dr Tania Gardner is an APA Pain Physiotherapist and senior physiotherapist in the Department of Pain Medicine, St Vincent’s Hospital Sydney. Tania has more than 25 years’ experience in the treatment of low back pain. She was integral in the establishment of the Reboot online program, and continues to be involved in the research and development of the program. She completed her PhD in 2017 investigating patient-led goals in chronic low back pain.
Additional contributions from APA NSW Pain Group chair Tim Austin, APA Pain Physiotherapist, registrar in Pain Specialisation TP; APA WA Pain Group chair Melanie Galbraith, APA Pain Physiotherapist; Michelle Wilson, APA Pain Physiotherapist; facilitators in TP Peter Roberts, FACP, and Lois Tonkin, APA Pain Physiotherapist; and APA national Pain Group chair, Honoured Member Dianne Wilson, APA Pain Physiotherapist.